

Lady-Marie Dawson-Malcolm brings both lived experience and professional expertise to our conversation around tetraplegia and accessibility. A former army physical training instructor, she sustained a spinal cord injury in 1992 when her baby was just six months old and has since built a life defined by resilience, advocacy and impact. Now Partnerships Coordinator at the Spinal Injuries Association, she has spent over a decade supporting people with spinal cord injuries while also working to improve access across transport, services and the built environment.
Recently, supported by Calvium and Regain, the charity for people who have become tetraplegic, Lady-Marie has completed an Inclusive Design course with National Register of Access Consultants (NRAC).
In this interview, Lady-Marie reflects on her journey, from navigating life as a new mother after injury to becoming a trusted voice in accessibility, and shares her insights on design, technology and what truly inclusive systems should look like.

Tetraplegia affects not just mobility, but every aspect of daily life. How do the realities of living with tetraplegia differ for women and girls compared to men, particularly in relation to personal care?
It can be incredibly challenging. When I first sustained my injury, I lost all independence and couldn’t use my hands. Things that were once completely private, like washing and dressing yourself, suddenly had to be done by a stranger. Even now, 34 years later, I rely on carers for everything. There’s very little privacy left and that’s something you have to come to terms with.
For women and girls, I think it can be especially difficult. It’s not just physically challenging, it can feel undignified – needing help to use the toilet, having personal care managed in bed by carers. The menstrual cycle adds another layer of complexity and, at times, embarrassment.
Those early stages are hard, but over time you begin to adjust; you realise this is your reality and you have to accept help. That doesn’t make it easy, but it does become more manageable with time and mindset.
There’s also the impact on how we see ourselves as women. Many of us struggle with self-image and may feel less attractive, or worry that we won’t be seen in the same way by others. There can be fears about relationships, whether we’ll find a partner, or whether having children is possible. In reality, our bodies are still capable in many ways. But emotionally, it takes time to believe that and to rebuild confidence.
From my experience, fewer women than men in this situation tend to be in relationships. Living without a partner, and facing life more independently, is something many of us have to navigate alongside everything else.
Girls with tetraplegia grow up navigating disability alongside gendered expectations about independence, appearance and care. What long-term impact does this have on confidence and identity?
As women, we naturally want to express ourselves through how we look. We enjoy dressing up, feeling confident and being seen as individuals – not defined by our wheelchair. But after acquiring a disability, that can become more complicated. Something as simple as going into a shop and buying clothes off the rack isn’t always possible.
Before my injury I loved high heels and dressing up. Afterwards, I was told things like, “You’ll need to wear a soft tracksuit because you have to be careful with your skin,” and “You’ll need to wear trainers.” So there’s a real shift; not just physically but in how you’re expected to present yourself.
Over time, I’ve come to terms with my disability and developed my own style. I work with a dressmaker now so I can design my own outfits. It allows me to feel confident and in control of how I present myself.
But I recognise that not everyone feels able to do that. From conversations I’ve had with other women, many struggle with low self-esteem. There’s often a sense of uncertainty, “What can I wear now? What suits me? What’s possible?”
One thing many of us develop after acquiring a disability is strong problem-solving skills. You have to find ways to make things work for you. For me, that meant finding a way to feel confident again, so that when I go out, people see me, not just the chair.

Photo: Sunrise Medical
In your experience, are women with tetraplegia taken less seriously when they raise concerns about their bodies or symptoms – and does this intersect with race?
When I first sustained my injury, I remember thinking: first, you’re female; second, you’re Black; third, you’re disabled – three strikes, you’re out. That was my mindset at the time, but over the years that has changed.
I haven’t seen overt racism in how people respond to me, or at least not in a way that’s been clearly expressed. If it has been there, it’s been very well hidden. What I have felt more strongly is the impact of disability on how seriously you’re taken.
Part of that is also how I choose to approach situations. I tend to look beyond other people’s perceptions and present myself in a way that encourages them to see me as I am. But there are definitely moments where assumptions surface – about race, identity, status.
For example, when I’ve been in hospital waiting rooms, watching staff come in looking around for “Lady-Marie,” I can tell straight away they’re not expecting me. There’s an assumption, tied up in the title, that they’re looking for a white woman.
Overall, though, the biggest barrier I’ve encountered has been linked to disability: how people perceive your capabilities, how seriously they take your concerns, and how quickly they make judgments.
What would a healthcare system designed with women and girls with tetraplegia at its centre look like; from hospital wards to community care?
At the moment, many aspects of care are simply not set up for us, which makes even routine procedures challenging.
During a recent mammogram, the equipment wasn’t designed with someone like me in mind, and as a result, I could only have a partial mammogram and it couldn’t give a complete picture of my health. That’s a clear example of how systems fail to accommodate our needs.
In hospital settings, there are often basic gaps in understanding and preparation. Many healthcare professionals approach care with a generalised mindset, but tetraplegia requires specific knowledge and specialist equipment. That lack of knowledge creates barriers and means we often have to be very assertive just to receive appropriate care, which isn’t always well received. We’re not trying to tell people how to do their jobs, we’re simply trying to help them understand our bodies and what we need.
A truly inclusive healthcare system would listen to us. It would ensure staff are trained, equipment is accessible and appropriate, and that our expertise in our own bodies is respected. It would remove the need for us to fight to be heard, and instead work with us as partners in our care.

Photo: Spinal Injuries Association
What do designers and planners consistently miss when they don’t involve disabled women in the design process?
Too often, disability is defined and designed by non-disabled people, which misses the full picture of what’s actually required.
If you don’t involve disabled women in the process from the beginning, you miss the lived experience; the practical knowledge of what works, what doesn’t, and what’s needed to make spaces genuinely accessible.
I recently carried out an access audit at a new building near the Olympic Park, and it highlighted just how many details get overlooked. Wheelchairs, for example, come in all shapes and sizes. When I arrived, I couldn’t press the button to open the automatic door, despite it being the designated accessible entrance.
Inside, the accessible toilet presented more barriers. The door required grip strength and there wasn’t enough usable space to turn properly, meaning I had to reverse out. There were bins fixed in the wrong places, obstructing movement, the support rail was too high, and power points were positioned in ways that made them inaccessible.
These aren’t complex problems, they’re issues of positioning and they show the same thing: the intention to be accessible may be there, but without involving disabled people, the execution falls short.
The solution is straightforward. Involve us early, listen to our experiences and work with us as stakeholders in the design process. This is how you create spaces that work for everyone.
In the built environment, digital tools are often used for way-finding, booking assistance or accessing services. How well do these systems work for people with limited mobility and sensation, and who is being left out?
For me, technology has been transformative. Developments like smartphones and voice assistants in particular have had a huge impact on my independence.
I’m not able to hold a phone in my hand in the way most people would, so being able to use voice control is essential. I can speak to my phone when I’m out, and at home I use Alexa for so many things – from controlling my TV to managing everyday tasks.
When I’m travelling or going out, I rely heavily on apps. I’ll use tools like Google Maps to plan my journey, and if I’m taking the train, I can book tickets through an app and have the e-ticket sent straight to my phone. That removes the need to queue at a station or rely on someone else to assist me, which gives me much more independence.
At their best, digital tools are incredibly empowering – they remove barriers and make everyday activities more accessible. The challenge is that not everyone is included in that design thinking. If systems don’t account for different access needs – such as limited hand function, reliance on voice control, or fatigue – they can quickly become unusable. If there’s no alternative or support in place, people can be excluded entirely.
So while technology has the potential to level the playing field, it only does so when accessibility is built in from the start. Otherwise, the very tools meant to increase independence can end up creating new barriers for the people who rely on them most.

Many digital accessibility tools assume a certain level of physical movement, vision or speech. How should designers rethink these assumptions when developing technology for people with tetraplegia?
A lot of technology still assumes that users can hold, tap, or swipe a device, but that simply isn’t the reality for many people with tetraplegia. This becomes even more complex when additional access needs are involved.
I know someone with tetraplegia who is also losing her sight and now struggling to use her computer. She asked me if there was any technology that could help, but that question alone highlights the gap. Too often, solutions don’t account for overlapping challenges.
Improvements are happening. Speech technology, for example, has come a long way, and with the rise of AI there’s real potential. But it’s not always reliable and there are still concerns around consistency and safety. It can’t be the only solution.
Designers should be thinking beyond touch-based interaction. Even small, alternative inputs can make a huge difference. I remember a Samsung device that allowed you to answer a call just by waving your hand over it like a magic wand, which is incredibly powerful.
It’s about rethinking interaction altogether. If a small movement, gesture, or non-contact input can replace the need for fine motor control, it opens up technology in a much more inclusive way. That means building in accessibility from the start, and designing it around the realities of how people actually move, communicate and interact with the world.
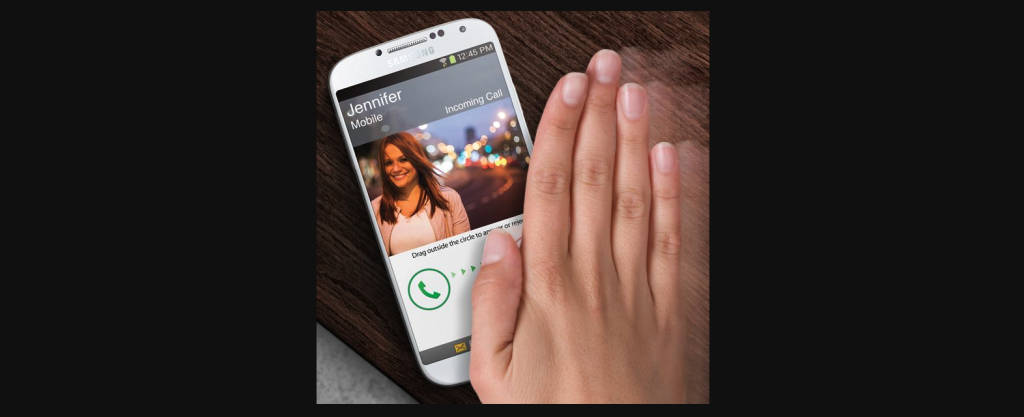
Photo: Samsung
Access to technology often depends on income, housing type and location. How does the digital divide affect disabled women and girls?
The digital divide has a very real impact on disabled women and girls, and one of the biggest factors is cost. Many of us simply don’t have the financial means to access the technology that would make our lives easier, unless we’ve received significant compensation for our disability.
When I first moved back into the community after my injury, I was supported by an assistive technology team who provided an environmental control system in my home. It included a simple remote that I could operate with a light tap of my hand, allowing me to turn lights on and off, answer the phone, and even open the door. That kind of technology is life-changing. It gives you independence and control over your environment.
But access to that support isn’t consistent. Funding is a challenge, and public bodies often require you to justify why you need certain equipment. There’s also the issue of affordability and scale; if a product is considered niche, it tends to be more expensive and less accessible. If designers and developers can create solutions that are more widely available and reasonably priced, it could make a significant difference to many people’s lives.
Inconsistency in provision is another problem. Access to support is often a postcode lottery and can depend heavily on where you live. Different local authorities have different priorities and budgets, which means one person might receive comprehensive support while another, with exactly the same level of injury and need, receives far less.
This isn’t equitable. Public bodies and property developers have a responsibility to address this by ensuring that accessible technologies are not only designed well, but are also available, affordable and distributed fairly.
Looking ahead, what would genuinely inclusive digital accessibility look like in homes, hospitals and public spaces; and who needs to be involved in designing it from the start?
Inclusive design isn’t just about creating the technology, it’s about ensuring it’s available, affordable, and distributed fairly. Everyone should have the same opportunities, options, and ability to choose what works best for them.
Whether you’re at home, in hospital, or in a public space, the experience should be seamless and supportive, not something you have to fight for or navigate differently depending on your postcode.
Just as importantly, the right people need to be involved in designing these systems – those who use them. There’s no point designing something based on assumptions about what might help, only to find it doesn’t work in practice and having to go back to the drawing board later.
Inclusion comes from listening, collaborating and ensuring that accessibility is not an afterthought, but a foundation.
You recently took an Inclusive Design course with NRAC. What did it involve, and in what ways has it expanded your understanding or introduced new viewpoints?
The course has been a real eye-opener for me. I’ve been involved in accessibility work for some time; advising on public transport with organisations like Network Rail, working with local authorities, and supporting efforts to make stations and services more accessible. But this course has taken that experience to another level and opened up a new chapter.
What really stood out was the sheer number of regulations that exist. There are detailed standards for everything – accessible toilets, tactile paving, bathrooms, and more. I hadn’t realised just how extensive it all is, and now, with greater awareness around neurodivergence and other access needs, that landscape is continuing to evolve.
The course has helped me to step back and see the bigger picture. As someone with tetraplegia, it’s natural to focus on my own lived experience, but this has broadened my perspective to better understand the needs of people with a wide range of disabilities. That’s been incredibly valuable, particularly when it comes to advising others.
It’s also reinforced the importance of getting things right from the start. If you design with accessibility in mind from the beginning, you avoid costly changes later on, and, more importantly, you create environments that actually work for people.
The course has really opened up a new chapter for me. It’s also given me the knowledge and confidence to contribute more formally to improving the built environment, whether that’s through access audits, advisory panels or future consultancy work.
Alongside my voluntary work, there’s potential for this to develop professionally. Ultimately, it’s about building credibility and ensuring that lived experience is recognised as expertise. This course is a step towards that, helping us to be heard, taken seriously and involved in shaping more inclusive spaces from the outset.
Thank you Lady-Marie for sharing your experience, perspectives and insights.
Contact us to discuss how digital innovation can support your goals.
Subscribe to the monthly Calvium newsletter to get more insight and inspiration like this in your inbox.



